
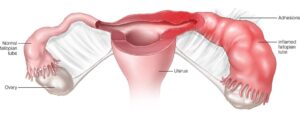
The female genital tract is prone to infection, it could be due to sexually transmitted or as a result of vaginal flora. A tubo-ovarian abscess or TOA is a complex infectious mass of the adnexa that forms as a consequence of pelvic inflammatory disease. Infection that affects the upper genital tract in women is called pelvic inflammatory disease or PID. The infection may involve a part or whole of the uterus, fallopian tubes and ovaries; this may also cause infection of the nearby pelvic organs. This infection may lead to tubo-ovarian abscess if left untreated. Apart from TOA, it may also cause endometritis, salpingitis, oophoritis, peritonitis, perihepatitis. A tubo-ovarian abscess can be defined as an inflammatory mass in the genital tract (ovary or fallopian tube), the mass thus forms has pus in its advanced stages. If the abscess has grown considerably, it may extend to neighboring pelvic organs such as bowel and bladder. However, tubo-ovarian abscess may also occur without pelvic inflammatory disease. Tubo-ovarian abscesses are generally found among women who is of reproductive age and generally result from upper genital tract infection. About 60% of the women with tubo-ovarian abscess are not sexually active, which means it affects them at a young age. More often than not, tubo-ovarian abscess is an offshoot of pelvic inflammatory disease.
What assumes significance is this infection should not be taken lightly as it can be life-threatening. Medical or surgical modalities have to be explored. If there is rupture of an abscess, it may lead to infection. With the introduction of modern treatment processes such as antibiotics and surgery, the mortality rate due to tube-ovarian abscess has come down significantly. However, in the olden days it was about 50%. Today the mortality rate is zero, if the abscess is not ruptured. Antibiotic regimen, drainage via minimally-invasive route, surgical procedure or a combination of these modalities is used to treat a tubo-ovarian abscess. If the abscess is not large, then it is likely to be resolved with antibiotic drug regimen.
Diagnosis of tubo-ovarian abscess:
If you are suffering from a tubo-ovarian abscess, you may show some or all of the following signs and symptoms:
- Adnexal tenderness (bilateral or unilateral)
- Cervical excitation
- Pyrexia
- Abnormal cervical or vaginal discharge
- Elevated white cell count
- Elevated erythrocyte sedimentation rate
- Elevated C‐reactive protein
- Chlamydia trachomatis test positive
- An adnexal mass on abdominal palpation
However if your TOA is severe, you may also suffer from tachycardia, hypotension, increased respiratory rate, raised lactate. Ninety percent of women with TOA may also have diarrhea and fever. White cell count is another indicator that throws light on the presence of TOA. It should be noted that the absence of a raised white cell count and fever does not exclude the presence of TOA. Above normal level of C-reactive protein with other clinical signs is a sensitive indicator of TOA. If the doctor is suspicious of a TOA, the doctor may order serum lactate and other blood cultures to exclude the condition. Screening for sexually transmitted infections is another important parameter in the diagnosis of tubo-ovarian abscess.
In order to diagnose the condition, the doctor may seek the help of some imaging techniques like ultrasound or CT. On an ultrasound scan, a tubo-ovarian abscess may appear as a solid or cystic mass. This can be present on either one side or both. However, the doctor may go in for further imaging such as a CT scan if the ultrasound is inconclusive or if some other pathology like appendicitis is suspected. A thick-walled, fluid-dense mass in the adnexa on CT scan is often signals a TOA.
Management of tubo-ovarian abscess:
Depending on the clinical and imaging findings, the doctor will adopt the first-line of management for a woman who is suspected to be suffering from this condition. If the condition is serious (if there are signs of infection), then it warrants immediate medical attention. Management of such a TOA may include prompt operative intervention and putting the patient on an antibiotic regimen. If the TOA is in the initial stage then the doctor may consider an antibiotic therapy and consider operative intervention only after a period of observation after the starting the drug therapy. Treating TOA with antibiotics has a success rate of 70% in women, though there is a high recurrence rate. Success of the antibiotic therapy depends on the ability of the drug to penetrate the abscess cavity and preventing it from recurring. Once there is an improvement and the patient has become clinically stable, the antibiotic regimen may be changed. Duration of the TOA treatment depends on the severity of the condition, if the condition is serious, a longer course is needed.
For enquiries related to Tubo Ovarian Abcess, or any other Gynae related issues, send a message to www.KJKHospital.com/contact



